The animal origin of 2019-nCoV is currently unclear: some early studies suggest a bat origin(1) while others postulate that snakes are the reservoir(2). It is known, however, that the infection likely spread at the Huanan seafood market, a “wet market” where live animals and meat are sold out in the open(3) (similar markets have been implicated in the creation of SARS). This market may have been the point where the virus crossed from another species to a human – the “spillover” event. The story of a zoonotic coronavirus causing global panic is hardly a new one, however: it has occurred twice before in the past two decades, first with SARS and then with MERS. Examining these epidemics may give us insight into the current situation.
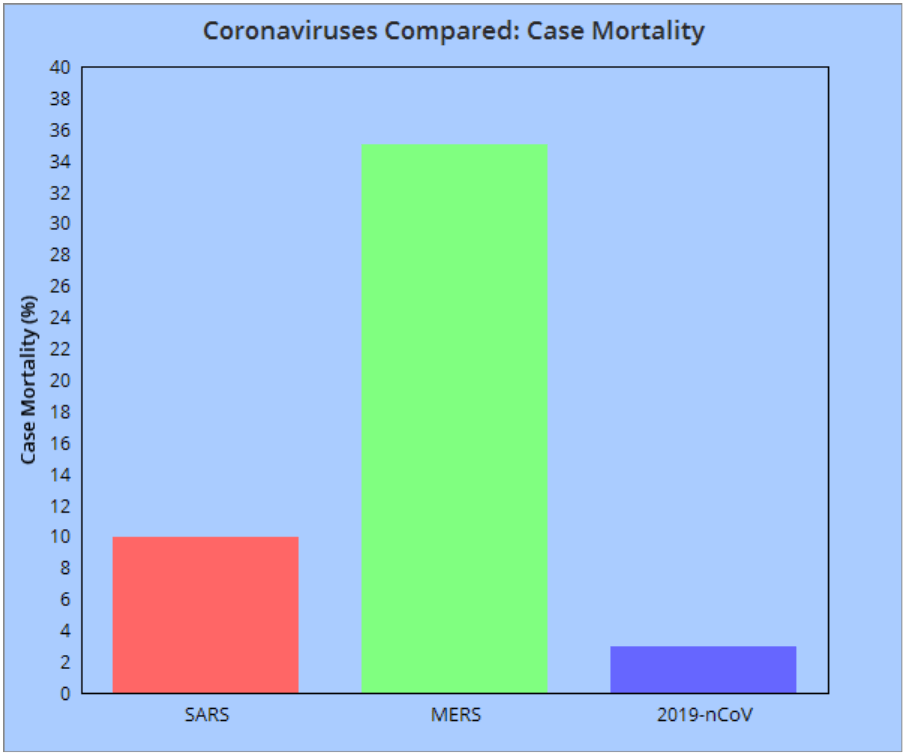
From 2002-2003, the World Health Organisation logged reports of 8096 probable cases of Severe Acute Respiratory Syndrome (SARS). This epidemic resulted in 774 deaths, with a case mortality rate of 9.6%. The coronavirus responsible was named SARS-CoV and was found to infect both the respiratory tract and gastrointestinal tract(4). The precise animal reservoir of this virus is unknown: it is possible that the virus transferred first from bats to civet cats and from there to humans. Infected patients suffered fevers, coughing, diarrhoea, headaches, and malaise, with severe cases eventually developing into respiratory distress. The epidemic began in the Guangdong province of China, with cases later reported in Toronto, Taipei, Hong Kong, Singapore, and Hanoi. An effective global response was mounted, with SARS no longer found in the wild, instead being confined to samples in research laboratories(5). Within a decade of this public health victory, however, a new coronavirus threat would emerge from a different part of the world…
In 2012, reports came in from Saudi Arabia of a new condition dubbed Middle East respiratory syndrome (MERS), caused by the coronavirus MERS-CoV. This infection has a case mortality rate of 35% (although WHO recognises that this may be an overestimate) but is difficult to transfer from person to person. Those providing care to a patient are most at risk (also true of SARS). Dromedary camels have been implicated as an animal reservoir of the virus, with animal-to-human transmission providing a source of fresh infections(6). Unlike SARS, MERS is still circulating in the wild: outbreaks are generally small, however, and MERS-CoV is not cause for much global concern. Comparing 2019-nCoV to SARS and MERS reveals some good news: as of current reports, 2019-nCoV’s case mortality rate appears to be lower than that of either MERS or SARS(7). The topic of infectivity will have to wait for another post: for 2019-nCoV, the R0 (a value related to the infectiousness of a disease) has not yet been decided (and deserves proper discussion in its own right).
So, dangerous zoonotic coronaviruses are nothing new, but, despite this, we are all still here: given that there is no vaccine or antiviral “cure” for these infections, only supportive treatments, how have we prevented deadly coronavirus pandemics? The deceptively simple (although by no means easy) answer is that we stopped people from transferring the virus to others. This included quarantines of infected individuals and screening at international airports, identifying sufferers before they could spread the virus to new locations. Public and health provider awareness of hygiene was also crucial, as was international scientific cooperation(8).
Perhaps, then, we are not so unprepared for this virus as the media suggests. Armed with our past experiences and current research, our healthcare providers, governments, and international agencies are already moving to deal with 2019-nCoV. As more information about the virus emerges over the coming weeks and months, we will learn how best it can be combatted and contained (stay tuned for more posts as the news happens). Discussing more about the exact properties of 2019-nCoV is beyond the scope of this post, so for the time being, remember: this is nothing new, and it probably isn’t the end of the world.
Author: Ben Dimbleby
References:
(1) Zhou P, Yang X, Wang X, Hu B, Zhang L, Zhang W, et al. Discovery of a novel coronavirus associated with the recent pneumonia outbreak in humans and its potential bat origin. bioRxiv 2020:2020.01.22.914952.
(2) Ji W, Wang W, Zhao X, Zai J, Li X. Homologous recombination within the spike glycoprotein of the newly identified coronavirus may boost cross-species transmission from snake to human. Journal of medical virology 2020 Jan 22,.
(3) Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet 2020 Jan.
(4) Andersson MI, Korsman SNJ, Zyl GV, Preiser W, Nutt L. Virology: an illustrated colour text. 2012; Available at: https://clinicalkeymeded.elsevier.com/#/books/9780323359528/cfi/6/116!/4/2/12/2/12/2/4/2@0:75.0.
(5) WHO. SARS (Severe Acute Respiratory Syndrome). Available at: https://www.who.int/ith/diseases/sars/en/. Accessed 28/01/, 2020.
(6) WHO. Middle East respiratory syndrome coronavirus (MERS-CoV). 2020; Available at: https://www.who.int/news-room/fact-sheets/detail/middle-east-respiratory-syndrome-coronavirus-(mers-cov). Accessed 29/01/, 2020.
(7) Mahase E. China coronavirus: what do we know so far? BMJ (Clinical research ed.) 2020 Jan 24,;368:m308.
(8) WHO. Chapter 5: SARS: lessons from a new disease. Available at: https://www.who.int/whr/2003/chapter5/en/index5.html. Accessed 28/01/, 2020. Accent 3;
