HIV and heart disease, two things we don’t necessarily think of as being intrinsically linked yet this is far from the truth. While in over the last 10 years, we have seen a decline life-threatening, opportunistic infections among treated HIV patients, this does not tell the whole story. In recent years clinicians have seen more and more instances of HIV related cardiovascular disease with it becoming the leading cause of death for patients with HIV (1).
Why is this the case? Scientists believe that the reason for patients with HIV having an increased risk of cardiovascular disease, with a HIV-positive person being twice as likely as a HIV-negative person to experience a heart attack or stroke (1), is due in part to the constant activation of the immune system. Although the mechanism behind this link is still being researched, it is suspected that due to the chronic activation of the immune system there is a surplus of inflamed blood vessels and clotting factors which both in turn function as major risk factors for serious cardiovascular events. This is seen event in medicated HIV patients where the levels of HIV are undetectable in the blood (2). This chronic inflammation is also linked to a build up of plaque in the arteries which is has also been linked to antiretroviral therapy, the current treatment of HIV, and many HIV-associated comorbidities such as drug abuse and opportunistic infections.
However there is hope, in 2015 the National Institute of Allergy and Infectious Disease and the National Heart, Lung and Blood Institute launched REPRIEVE (Randomised Trial to Prevent Vascular Events in HIV) which hopes to enrol a minimum of 6,500 HIV positive patients between the ages of 40 and 75 to see if a daily dose of pitavastatin can further reduce the risk of a cardiovascular event in people with HIV (3). This is the first major Phase 3 trial on this subject and will hopefully help further improve the quality of care provided as HIV transitions to chronic condition from the acute infection it once was.
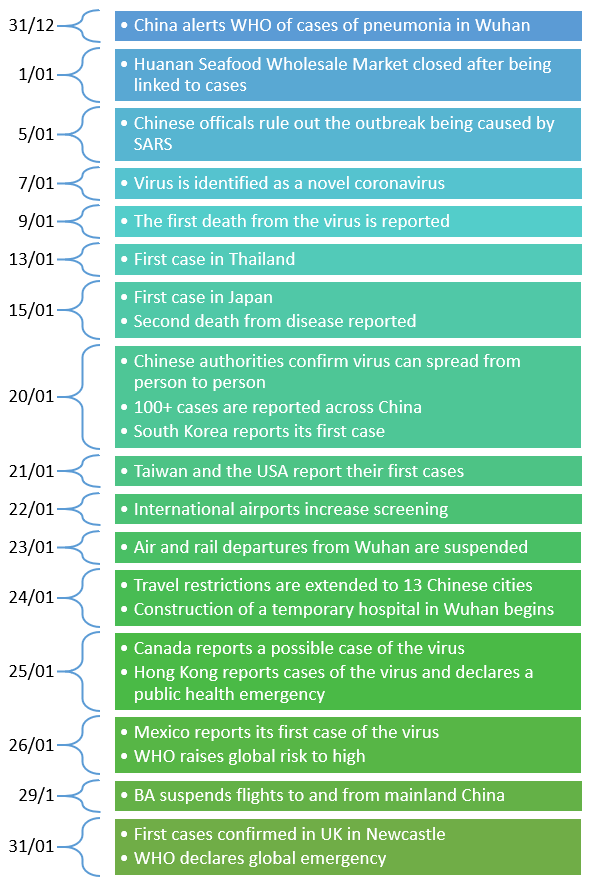
With more news breaking on the virus situation every day, it is worth taking a moment to step back and consider how we got here. The events leading up to the current moment are summarised here in a timeline showing snapshots of the discovery, spread, and response to 2019-nCoV:
Data from (1), (2), (3)
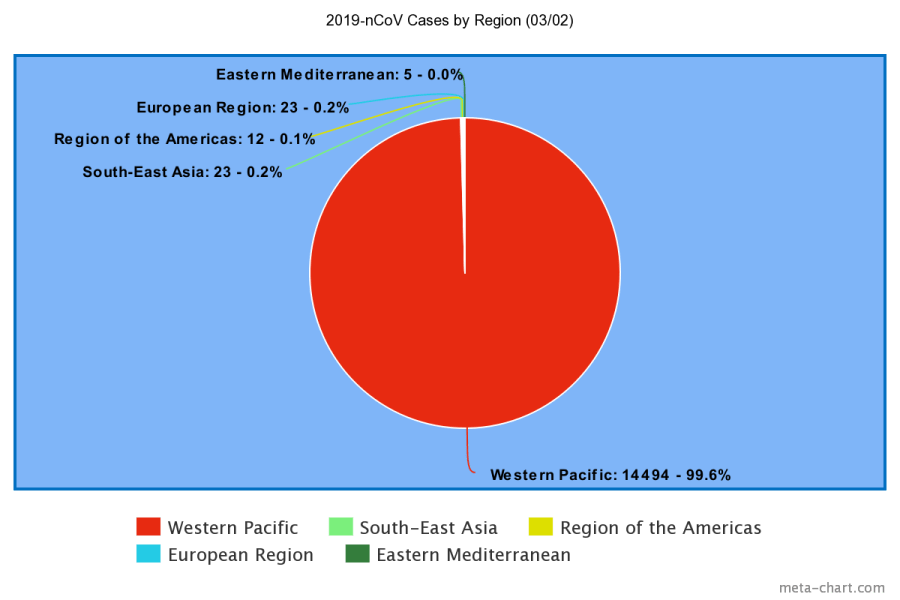
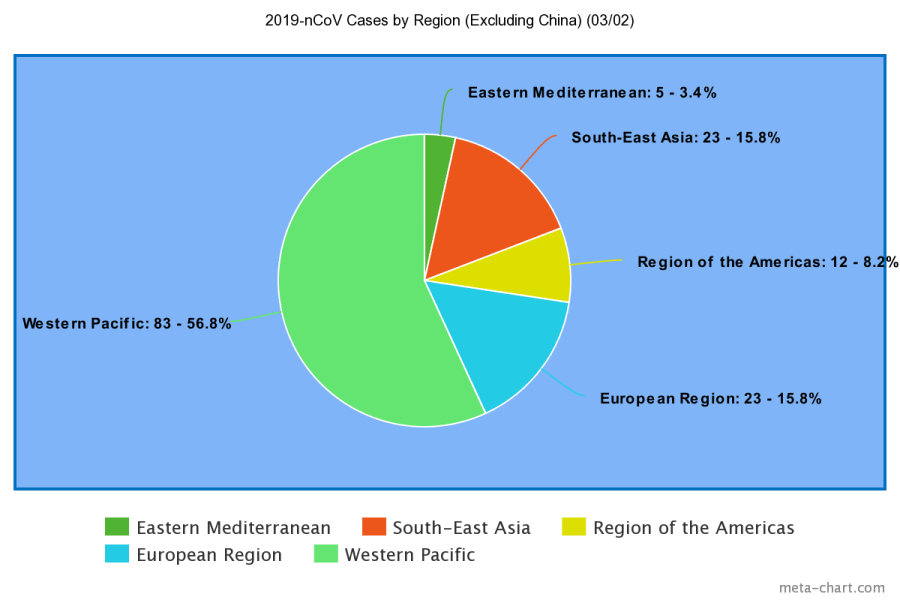
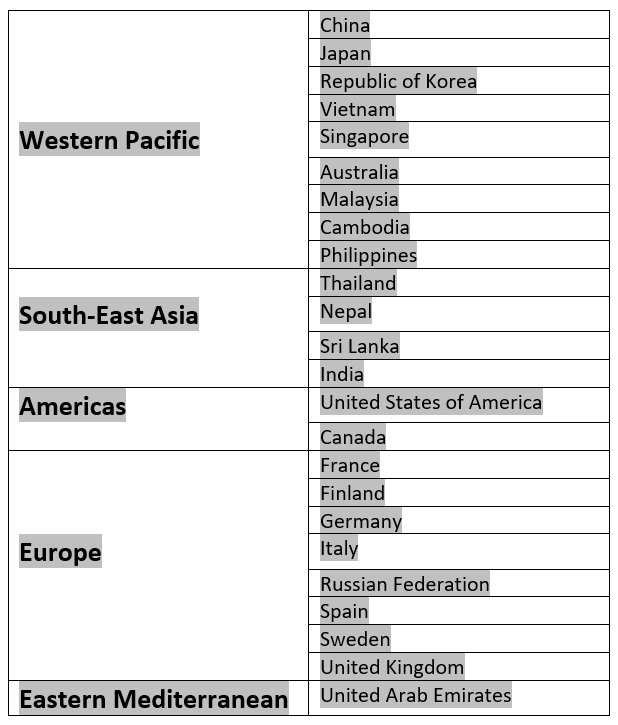
The number of reported cases has grown rapidly in recent weeks, both in number and in geographical location. Below are two charts summarising the number and location of these cases (note that as China accounts for the vast majority of cases, 14411, one chart includes China under the category of “Western Pacific” while the other chart excludes it, allowing comparison of other regions). The countries within each region that have reported cases are listed in a table.
Data from WHO (4)
This data gives us an idea of the increasingly global spread of the virus but also emphasises that the vast majority of cases are still within the borders of China. Look out for further posts to keep you updated on the situation.
The animal origin of 2019-nCoV is currently unclear: some early studies suggest a bat origin(1) while others postulate that snakes are the reservoir(2). It is known, however, that the infection likely spread at the Huanan seafood market, a “wet market” where live animals and meat are sold out in the open(3) (similar markets have been implicated in the creation of SARS). This market may have been the point where the virus crossed from another species to a human – the “spillover” event. The story of a zoonotic coronavirus causing global panic is hardly a new one, however: it has occurred twice before in the past two decades, first with SARS and then with MERS. Examining these epidemics may give us insight into the current situation.
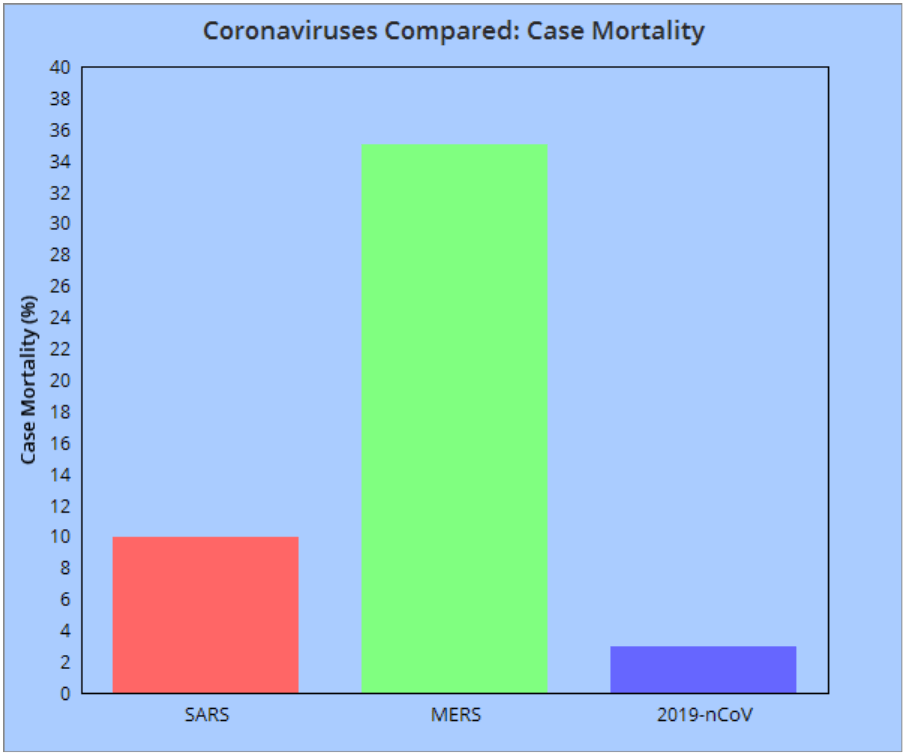
From 2002-2003, the World Health Organisation logged reports of 8096 probable cases of Severe Acute Respiratory Syndrome (SARS). This epidemic resulted in 774 deaths, with a case mortality rate of 9.6%. The coronavirus responsible was named SARS-CoV and was found to infect both the respiratory tract and gastrointestinal tract(4). The precise animal reservoir of this virus is unknown: it is possible that the virus transferred first from bats to civet cats and from there to humans. Infected patients suffered fevers, coughing, diarrhoea, headaches, and malaise, with severe cases eventually developing into respiratory distress. The epidemic began in the Guangdong province of China, with cases later reported in Toronto, Taipei, Hong Kong, Singapore, and Hanoi. An effective global response was mounted, with SARS no longer found in the wild, instead being confined to samples in research laboratories(5). Within a decade of this public health victory, however, a new coronavirus threat would emerge from a different part of the world…
In 2012, reports came in from Saudi Arabia of a new condition dubbed Middle East respiratory syndrome (MERS), caused by the coronavirus MERS-CoV. This infection has a case mortality rate of 35% (although WHO recognises that this may be an overestimate) but is difficult to transfer from person to person. Those providing care to a patient are most at risk (also true of SARS). Dromedary camels have been implicated as an animal reservoir of the virus, with animal-to-human transmission providing a source of fresh infections(6). Unlike SARS, MERS is still circulating in the wild: outbreaks are generally small, however, and MERS-CoV is not cause for much global concern. Comparing 2019-nCoV to SARS and MERS reveals some good news: as of current reports, 2019-nCoV’s case mortality rate appears to be lower than that of either MERS or SARS(7). The topic of infectivity will have to wait for another post: for 2019-nCoV, the R0 (a value related to the infectiousness of a disease) has not yet been decided (and deserves proper discussion in its own right).
A comparison of the case mortality rates of the viruses. Note that 2019-nCov’s mortality is likely to change as more data is released. Data from BMJ (7).
So, dangerous zoonotic coronaviruses are nothing new, but, despite this, we are all still here: given that there is no vaccine or antiviral “cure” for these infections, only supportive treatments, how have we prevented deadly coronavirus pandemics? The deceptively simple (although by no means easy) answer is that we stopped people from transferring the virus to others. This included quarantines of infected individuals and screening at international airports, identifying sufferers before they could spread the virus to new locations. Public and health provider awareness of hygiene was also crucial, as was international scientific cooperation(8).
Perhaps, then, we are not so unprepared for this virus as the media suggests. Armed with our past experiences and current research, our healthcare providers, governments, and international agencies are already moving to deal with 2019-nCoV. As more information about the virus emerges over the coming weeks and months, we will learn how best it can be combatted and contained (stay tuned for more posts as the news happens). Discussing more about the exact properties of 2019-nCoV is beyond the scope of this post, so for the time being, remember: this is nothing new, and it probably isn’t the end of the world.
Author: Ben Dimbleby
References:
(1) Zhou P, Yang X, Wang X, Hu B, Zhang L, Zhang W, et al. Discovery of a novel coronavirus associated with the recent pneumonia outbreak in humans and its potential bat origin. bioRxiv 2020:2020.01.22.914952.
(2) Ji W, Wang W, Zhao X, Zai J, Li X. Homologous recombination within the spike glycoprotein of the newly identified coronavirus may boost cross-species transmission from snake to human. Journal of medical virology 2020 Jan 22,.
(3) Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet 2020 Jan.
Are the end times upon us? Reading the reports from the media, you may be led to believe so: unscrupulous sources depict a dangerous super-plague originating from Wuhan, promising annihilation on a global scale. The true story of this new coronavirus, however, is more complex and (unsurprisingly) less sensational: it is a story of epidemics past and present, of political lessons learned, and of public health lessons neglected.
To simply call the novel virus present in Wuhan “coronavirus” is an oversimplification. The term coronavirus refers, in fact, to an entire family of viruses, most of which cause little more than “the sniffles” and a sore throat in healthy people. Most coronaviruses only spread to the lower respiratory tract in a few individuals (due to the viruses’ preference for lower temperatures). Given that coronaviruses cause 2-10% of common colds(1), many of us will already have experienced the effects of one!
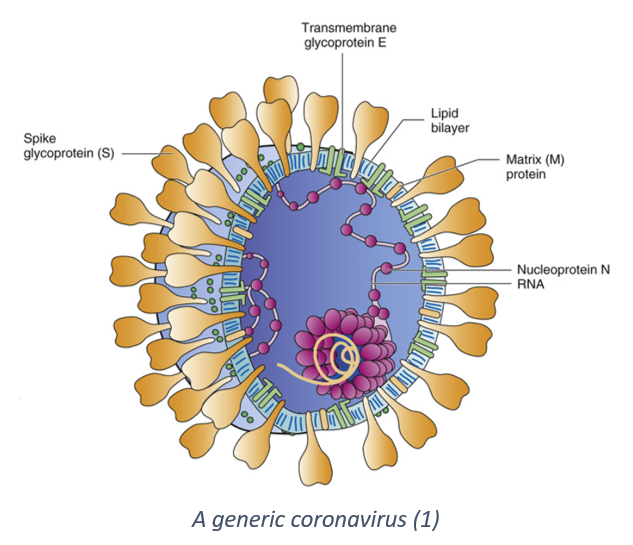
The name “coronavirus” comes from the appearance of the viruses: club-like glycoproteins protrude from their lipid bilayer, giving them the appearance of having a “crown” (a corona in Latin). It is these E2 protein “spikes” that have a role in binding to human cells. The coronavirus family has a single-stranded positive-sense RNA genome that, upon infecting a cell, is first translated by host cell ribosomes to form a viral RNA polymerase and other proteins. Using this polymerase, negative-sense RNA templates are produced: from these templates, new viral genomes are replicated and mRNAs coding for individual viral proteins can be created. The host cell assembles the virus and a new virion is born. Coronavirus infection is cytolytic, meaning it causes cell destruction, and is spread from person to person by fluid droplets and aerosols (after all, coughs and sneezes spread diseases!)(2).
Infection by a common coronavirus is a minor event for most people: their immune systems quickly fend off this cellular invader, with the host only experiencing some upper respiratory tract symptoms such as sneezing and a sore throat. Clearly, then, this new coronavirus (named 2019-nCoV,meaning “2019 Novel Coronavirus”) is something a little outside of the ordinary; it causes pneumonia, an inflammation of the lung tissues, and is associated with a rising number of deaths. So why is this new virus more dangerous than its relatives? The answer lies in its origin: this novel virus is zoonotic(3), meaning that it has crossed from another species to humans. As a result, the virus has different properties to those normally found in our populations and so causes greater illness and mortality in humans. It seems likely that 2019-nCoV is most dangerous to vulnerable individuals such as those with respiratory disease and the elderly.
So, we have discussed the general nature of coronaviruses and seen why 2019-nCoV is unusually dangerous. Next, we will consider exactly what and where the origin of the virus may have been, and discover why it may not be so unusual after all…
(3) Ji W, Wang W, Zhao X, Zai J, Li X. Homologous recombination within the spike glycoprotein of the newly identified coronavirus may boost cross-species transmission from snake to human. Journal of medical virology 2020 Jan 22,.